So, how much time do you spend doing paperwork? Assessments, progress notes, treatment plans, billing, updates, etc.–the lot?
When I asked the director of the agency I was working at last week, it took him no time to respond. “Fifty percent,” he said, then added without the slightest bit of irony, “It’s a clinic-wide goal, keeping it to 50% of work time.”
Truth is, it’s not the first time I’ve heard this figure. Wherever I travel–whether in the U.S. or abroad–practitioners are spending more and more time “feeding the bureaucratic beast.” Each state or federal agency, regulatory body, and payer wants a form of some kind. Unchecked, regulation has lost touch with reality.
Just a few short years ago, the figure commonly cited was 30%. In the last edition of The Heart and Soul of Change, published in 2009, we pointed out that in one state, “The forms needed to obtain a marriage certificate, buy a new home, lease an automobile, apply for a passport, open a bank account, and die of natural causes were assembled … altogether weighed 1.4 ounces. By contrast, the paperwork required for enrolling a single mother in counseling to talk about difficulties her child was experiencing at school came in at 1.25 pounds” (p. 300).
Research shows that a high documentation to clinical service ratio leads to higher rates of:
- Burnout and job dissatisfaction among clinical staff;
- Fewer scheduled treatment appointments;
- No shows, cancellations, and disengagement among consumers.
Some potential solutions have emerged. “Concurrent ,” a.k.a., “collaborative documentation.” It’s a great idea: completing assessments, treatment plans, and progress notes together with clients during rather than after the session. We started doing this to improve transparency and engagement at the Brief Family Therapy Center in Milwaukee, Wisconsin back in the late 1980’s. At the same time, it’s chief benefit to date seems to be that it saves time on documentation–as though filling out paperwork is an end in and of itself!
Ostensibly, the goal of paperwork and oversight procedures is to improve accountability. In these evidence-based times, that leads me to say, “show me the data.” Consider the wide-spread practice–mandate, in most instances–of treatment planning. Simply put, it is less science than science fiction. Perhaps this practice improves outcomes in a galaxy far, far away but on planet Earth, supporting evidence is spare to non-existent. Where is the evidence that any of the other documentation improves accountability, benefits consumers, or results in better outcomes?
Put bluntly, the field needs an alternative. What practice not only insures accountability but simultaneously improves the quality and outcome of behavioral health services? Routinely and formally seeking feedback from consumers about how they are treated and their progress.
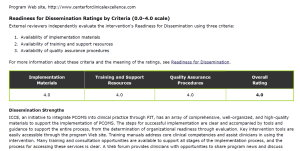
Soliciting feedback need not be time consuming nor difficult. Last year, two brief, easy-to-use scales were deemed “evidence-based” by the Substance Abuse and Mental Health Services Administration (SAMHSA). The International Center for Clinical Excellence received perfect scores for the materials, training, and quality assurance procedures it makes available for implementing the measures into routine clinical practice:
![]()
Then again, these two forms add to the paperwork already burdening clinicians. The main difference? Unlike everything else, numerous RCT’s document that using these forms increases effectiveness and efficiency while decreasing both cost and risk of deterioration.
Learn more at the official website: www.whatispcoms.com. Better yet, join us in Chicago for our upcoming intensives in Feedback Informed Treatment and Supervision:


In the meantime, would you please let me know your thoughts? To paraphrase Goldilocks, is the amount of documentation you are required to complete, “Too much,” Too little,” or “Just about Right!” Type in your reply below!