I’m not sure what was going on in our field last week. From the emails I received, it seemed something big — no, monumental. Here are just a handful of the highlights:
“The single modality that’s transforming how clinicians do therapy … and making them so successful.”
A new approach for “Getting to the heart of complex and deep-rooted clinical issues, fast.”
A “unique and integrative approach for … building thriving relationships that last!”
You will learn to offer “transformative trauma healing results … [and] become the go-to trauma healer.”
Plus, certifications in “complex trauma, PTSD, and dissociation,” “polyvagal therapy,” and — no irony intended — “Narcissistic Abuse Treatment Clinician.”
Now, truth is, I get a lot of email. On any given day, a certain percentage of what lands in my inbox is made up of solicitations. A couple of advertisements for training in this or that therapy would, therefore, have gone unnoticed.
This was different. One day alone I received 41 separate come-ons — all with the same bold promises and time-limited discounts for “special customers” like me.
I still don’t know what led to the deluge. What is certain is that it had nothing to do with advances in the “science of psychotherapy.” Over the last 50 years, treatment methods have proliferated despite a lack of evidence of differential effectiveness between approaches. And even when a randomized controlled trial indicates a particular approach works, none show practitioners become more effective when they are trained in that modality.
Consider a study out of the United Kingdom (1). There, massive amounts of money have been spent training clinicians to use cognitive behavioral therapy (CBT). Clinicians participated in a high intensity course that included more than 300 hours of training, supervision, and practice. Competency in delivering CBT was assessed at regular intervals and shown to improve significantly over the course of the training program. And yet, despite the tremendous investment of time, money, and resources, outcomes did not improve. In short, clinicians were as effective as they’d been before being trained.
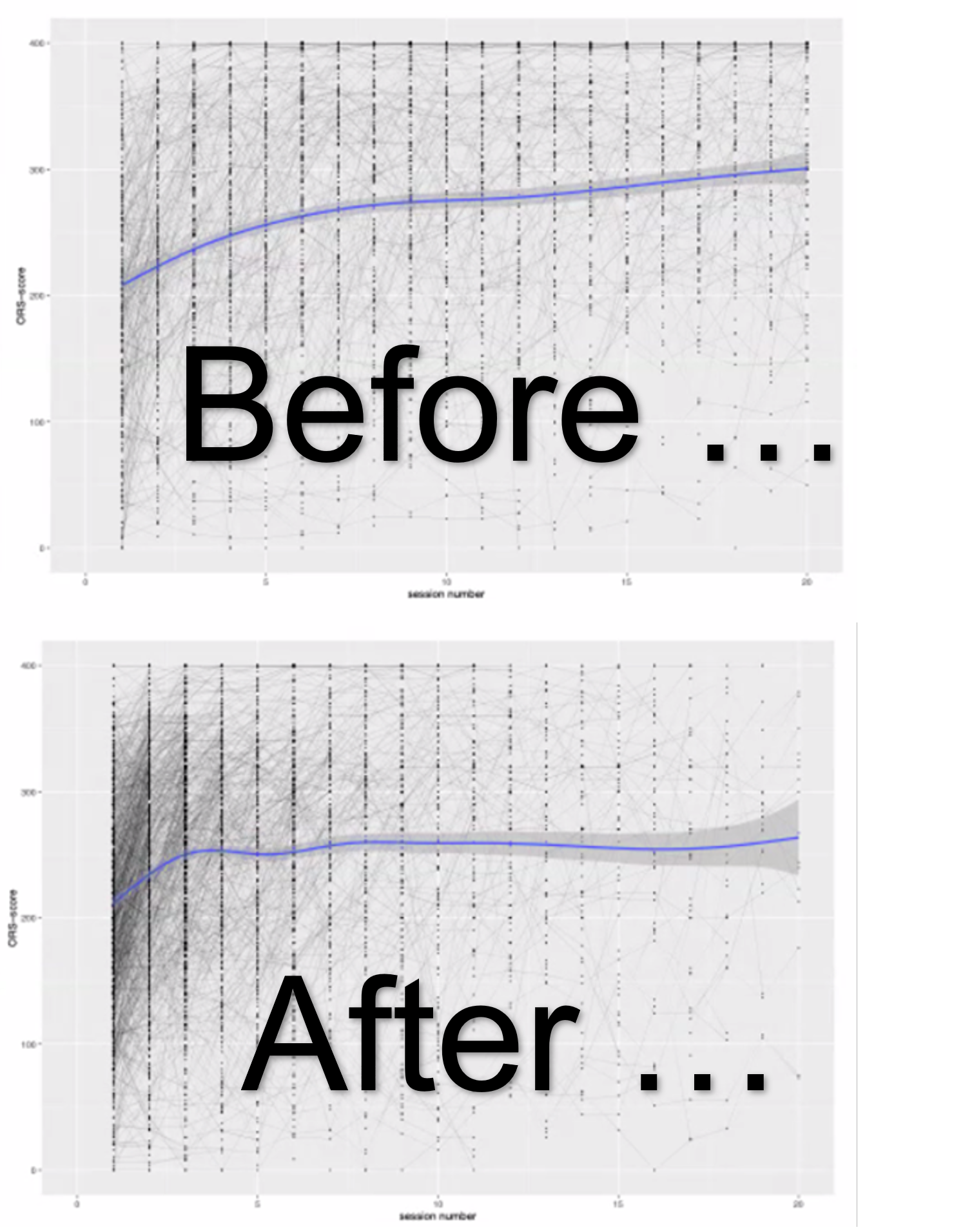
Contrast the field’s relentless pursuit of “treatment technology” with the work of psychologist Timothy Anderson. A decade-and-a-half ago, he developed a tool for measuring therapists’ interpersonal skills. Known as The Facilitative Interpersonal Skills Performance Task (FIS), it assesses a range of abilities (e.g., warmth, empathy, verbal fluency, hope, emotional expression and persuasiveness) by rating therapist responses to video simulations of challenging client-therapist interactions. It turns out that therapists who perform well on the FIS establish stronger relationships and are more effective (2). More to the point, the evidence shows FIS-related skills are trainable and that such training leads to better results (3, 4, 5).
Next month, I’ll be posting a summary of a study my colleagues and I just published documenting the impact of using deliberate practice to improve interpersonal skills — namely, empathy (You won’t be surprised to learn that clinicians’ assessment of their abilities did not correlate with their actual performance).
In the meantime, take a listen to the interview below with Dutch researchers, Sabine van Thiel and Kim de Jong. Their recently published study identified multiple, different types of therapist FIS response styles — including the elusive, “supershrink.”
Until next time,
Scott
Director, International Center for Clinical Excellence
P.S.: The final fireside chat with me and Daryl Chow is scheduled for the last Tuesday of this month. It’s free, of course, but you must register to secure a spot. Click here.